As someone who has worked in LGBTQ+ health research and innovation for a decade while also living and volunteering as a member of the queer community, sometimes I am in a position to notice gaps between academic evidence and community wisdom. In an ideal world, the two would match and reinforce each other. However, research can be slow to capture the richness of lived experience, and community knowledge isn’t always valued or empirically validated by the research establishment.

These gaps often point to an opportunity to expand knowledge and improve health. A key part of Eidos’ mission, and a rewarding part of my job, is bringing people together around these opportunities to create new potential for wellbeing that’s grounded in lived experience and data. By gathering people from different walks of life and pooling our unique perspectives, we become more likely to not just see the gaps but to collectively imagine bridges across them.
What Communities Understand: Our Common Need for Shared Experience and Identity
One gap that I have come to see clearly is how much more central peer connection is in community spaces than in academic ones. Look at the offerings of your local LGBTQ+ center or other community serving organization:
- youth programming
- elder initiatives
- recovery meetings
- women’s circles
- identity-based support groups
The backbone programs of community organizations are all built on the unspoken understanding that connecting around shared identity and experience is essential to thriving.
As a volunteer peer support counselor at my local LGBTQ+ community center, I have witnessed the need for connection firsthand. Amid the political hostility, funding cuts, and shrinking institutional support of the last year — particularly affecting trans and BIPOC communities — LGBTQ+ people have turned to queer networks of mutual aid and peer support to fill the gaps.
People come seeking help with workplace discrimination, coming out to family, finding affirming care, housing, or legal support. Underneath the various material needs, they also come seeking connection. They want help navigating their life circumstances from someone who understands — someone who can reflect their dignity, experience, and identity back to them.
I bet this instinct feels familiar to each of us. When I first came to terms with being queer, the first thing I did was reach out to a friend who had done the same years earlier. I remember asking some version of “how do I do this?” I didn’t just want advice. I wanted advice from someone who understood what it was like to be in my shoes. And this isn’t unique to the LGBTQ+ community.
There is a particular kind of support we all need at times that is based on shared experience or identity, when the key to our wellbeing is not just the solution to a problem but assurance that someone like us has overcome it before and is here with us now.
This need is deeply ingrained in queer community experiences and foundational to the way we give and receive support.
The Gap: Limited Investment in Peer-focused Research and Care
While peer connection is central to many community programs, it has historically played a much smaller role in research and healthcare. If you seek out peer support in a healthcare setting, you are likely to find only two kinds. The first kind is mental health and substance use recovery support provided by a certified peer support specialist. These professionals use their own lived experience in recovery as well as basic, standardized training in mental health support as part of care teams.
Second, if you are diagnosed with cancer and seek care at a large cancer center, you may be able to find a support group for individuals with the same diagnosis. Beyond these two applications, shared lived experience largely remains unleveraged in healthcare.
While there is some research on peer support, it is spread across multiple fields and technical concepts, leaving big gaps in what we can empirically say about its ability to impact health. For instance, how can we compare a study on peer support specialists’ ability to improve substance use recovery outcomes, to a study on the impact of a local Gay Student Alliance on LGBTQ+ students’ academic success?
Those contexts, outcomes, and applications of peer support are so different that it’s hard to say if their findings tell the same story. Scientific certainty requires repeating the same test with the same conditions and getting the same result. There simply hasn’t been enough repetition of findings in this area to build a coherent case for shared lived experience.
That said, the research that does exist can give us some signal about whether there’s anything to the community wisdom about peer connection’s value, and whether more investigation is warranted. First, studies do document the community intuition that queer people turn toward each other instinctively when seeking help. For example:
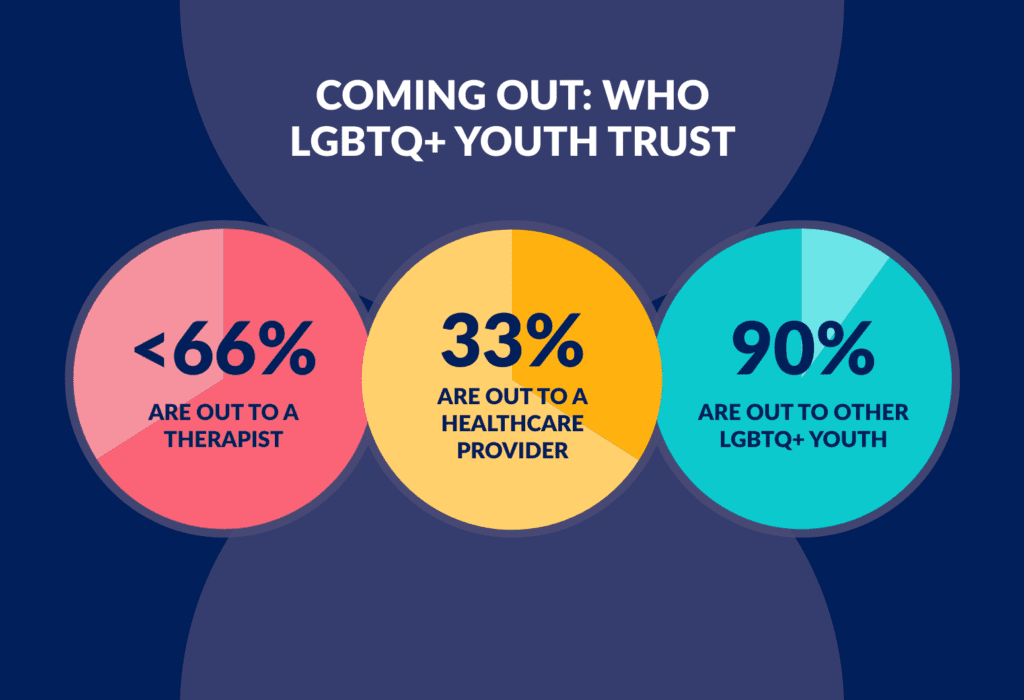
- Less than two-thirds of LGBTQ+ youth are out to a therapist, and only one-third are out to a health care provider, but over 90% are out to other LGBTQ+ youth. 1
- When seeking support on social media, Black and Hispanic LGBTQ+ young adults prefer connecting with users who share their sexuality, gender, and racial and ethnic identities, saying that support feels safer and more tailored to their experience.2
- LGBTQ+ adults say that they consider healthcare providers’ sexuality, gender, and race when searching for care, and that they feel safer with providers who share their identities. 3, 4, 5
Second, studies also back up the community assumption that there is good to be found in peer connection. Multiple studies have demonstrated that peer support contributes to health and wellbeing:
- Peer support specialists positively impact patient treatment engagement, empowerment, hope, social connection, and quality of life.6 And the benefits appear greatest for vulnerable populations.7
- LGBTQ+ youth with mentors are more likely to graduate high school and college8 and are more likely to maintain hopefulness about the future, despite experiences of harassment or stigma.9
- Perceived support from peer support groups like Gay Straight Alliances is associated with higher self-esteem and wellbeing among LGBTQ+ youth.10
- Having core confidants who can provide health-related decision support is associated with greater wellbeing among LGBTQ+ elders.11

The evidence, though limited, affirms that community organizations haven’t centered peer support by accident. They’ve done it because they see that it matters to people and provides a benefit that the research and healthcare worlds have not fully appreciated. They point us to an opportunity to leverage peer connection as a tool for health and wellbeing, to build a body of evidence to better support its effects and scalability.
Eidos’ Peer Mentoring Work: Building on the Evidence
At Eidos, we have been interested in doing just that: building the case for LGBTQ+ peer support as a tool to address the effects of marginalization, stigma, and ultimately improve queer health and wellbeing. Specifically, Dr. José Bauermeister has forged research partnerships to test whether peers can deliver existing, evidence-based interventions known to improve physical and mental health outcomes, opening the potential that peers could extend the capabilities and scale of existing health care treatments.
One example is the iReach study,12 which trained young adult peer mentors to support young men who have sex with men (YMSM) in building life skills and setting health-related goals. Peer mentors were trained in Motivational Interviewing (MI), a well-established counseling approach, and supported participants in identifying their own goals and motivations. With training and supervision, peer mentors demonstrated skills comparable to those of mental health clinicians.13
Building on this work, the Supporting Transitions to Adulthood and Reducing Suicide (STARS) pilot study explored whether peer mentors could strengthen the impact of suicide prevention tools.14 In this study, peer mentors supported LGBTQ+ young adults in using safety plans and coping strategies—tools that are evidence-based and effective but often underused. By helping participants keep these safety plans relevant and accessible, peer mentors supported more consistent use. Early results show that participants reported greater use of safety plans and reduced suicidal thoughts after two months.

The Opportunity: Working Together to Leverage Peer Support
Taken together, community wisdom and a growing body of data point to the untapped potential of peer connection to support health. The evidence suggests that weaving shared experience and peer support into our work can increase our reach and impact. It begs the question, where might peer connection already exist – or be missing – in the work we are doing? And it leaves space for countless answers that allow health services to integrate new peer applications or to equip existing peers with evidence-based tools to maximize their ability to support health and wellbeing.
At Eidos, we’re interested in continuing to test, strengthen, and scale peer-led approaches, and to bringing together people and teams from different professional backgrounds to bridge from potential to impact.
If you’re experimenting with peer support, wondering how it might fit your setting, or interested in building the evidence together, I’d love to connect. Send an email to eidos@nursing.upenn.edu or send me a message through our website contact form.
